 View normal meseteric fixation.
View normal meseteric fixation.Note the broad fan of meseteric attachment of the small bowel making it difficult for a volvulus of the small bowel to occur.
If the correct rotation does not occur, it is termed "malrotation". This results in the failure of proper mesenteric development so that instead of a broad fan of mesenteric attachment, the entire midgut is attached to the posterior abdominal wall by a short, narrow stalk in the region of the duodenum. There may also be bands crossing the duodenum (Ladd's Bands) which can cause duodenal obstruction.
 View malrotation and Ladd's bands.
View malrotation and Ladd's bands.
Note the mesenteric attachment of the cecum. This narrow stalk is more prone to volvulus. Additionally, this stalk (Ladd's bands) is capable of compressing the duodenum and obstructing it.
In a malrotation, many meters of intestine are free to twist around this stalk, which, since it contains the superior mesenteric artery, is vulnerable to strangulation and ischemic necrosis. The occurrence of this twisting and strangulation results in the surgical emergency called midgut volvulus. Midgut volvulus should not be confused with cecal or sigmoid volvulus. Cecal and sigmoid volvulus generally occur in adults. Sigmoid volvulus involves the large bowel and can often be decompressed by barium enema or other non-surgical procedures.
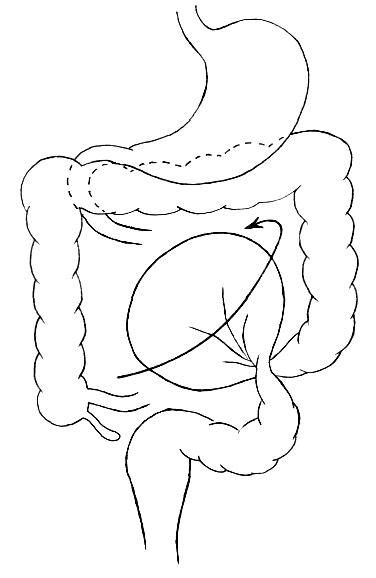
 VIew midgut volvulus.
VIew midgut volvulus.In midgut volvulus, the majority of the small bowel is involved in the stragulation. Substantial small bowel necrosis occurs without prompt surgical intervention.
 View cecal volvulus.
View cecal volvulus.
In malrotation, the cecum may be prone to twisting or kinking if it is excessively mobile. Cecal volvulus can occur in the absence of malrotation. This most often presents in adults rather than children.
 View sigmoid volvulus.
View sigmoid volvulus.Sigmoid volvulus is the most common site of colonic volvulus. It occurs most often in the elderly. It is associated with elongation of the descending colon making the sigmoid region hypermobile and prone to twisting.
没有评论:
发表评论